Abstract
Background: Dead space is the volume not taking part in gas exchange and, if increased, could affect alveolar ventilation if there is too low a delivered volume. We determined if there were differences in dead space and alveolar ventilation in ventilated infants with pulmonary disease or no respiratory morbidity.
Methods: A prospective study of mechanically ventilated infants was undertaken. Expiratory tidal volume and carbon dioxide levels were measured. Volumetric capnograms were constructed to calculate the dead space using the modified Bohr-Enghoff equation. Alveolar ventilation (VA) was also calculated.
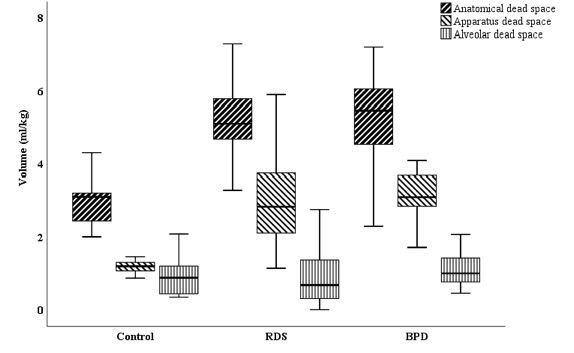
Results: Eighty-one infants with a median (range) gestational age of 28.7 (22.4–41.9) weeks were recruited. The dead space [median (IQR)] was higher in 35 infants with respiratory distress syndrome (RDS) [5.7(5.1-7.0) ml/kg] and in 26 infants with bronchopulmonary dysplasia (BPD) [6.4(5.1–7.5) ml/kg] than in 20 term controls with no respiratory disease [3.5(2.8–4.2) ml/kg, p<0.001]. Minute ventilation was higher in both infants with RDS or BPD compared to the controls. VA in infants with RDS or BPD was similar to that of the controls [p=0.54].
Conclusion: Prematurely born infants with pulmonary disease have a higher dead space than term controls, which may influence the optimum level during volume targeted ventilation.
Methods: A prospective study of mechanically ventilated infants was undertaken. Expiratory tidal volume and carbon dioxide levels were measured. Volumetric capnograms were constructed to calculate the dead space using the modified Bohr-Enghoff equation. Alveolar ventilation (VA) was also calculated.
Results: Eighty-one infants with a median (range) gestational age of 28.7 (22.4–41.9) weeks were recruited. The dead space [median (IQR)] was higher in 35 infants with respiratory distress syndrome (RDS) [5.7(5.1-7.0) ml/kg] and in 26 infants with bronchopulmonary dysplasia (BPD) [6.4(5.1–7.5) ml/kg] than in 20 term controls with no respiratory disease [3.5(2.8–4.2) ml/kg, p<0.001]. Minute ventilation was higher in both infants with RDS or BPD compared to the controls. VA in infants with RDS or BPD was similar to that of the controls [p=0.54].
Conclusion: Prematurely born infants with pulmonary disease have a higher dead space than term controls, which may influence the optimum level during volume targeted ventilation.
| Original language | English |
|---|---|
| Journal | Pediatric Research |
| Publication status | Published - 2022 |
{kind=link}